
Ruptured cranial (or anterior) cruciate ligament is one of the most common causes of hind limb lameness in dogs.
The cruciate ligaments are the two most important stabilizers of the knee joint. Although the knee joint of dogs and humans looks similar, in humans, the hip, knee and ankle joints are parallel to each other and perpendicular to the weight bearing surface (foot). This allows us to stand easily without any stress on any ligaments. Dogs however, stand on their toes with their ankles up in the air and their knees bent forward. The top weight bearing surface of the tibia (shin bone) slopes backwards. Weight bearing creates forces that push the femur back down the sloping tibial plateau. The main structure stopping the femur moving back is the cranial cruciate ligament.
With every step the dog takes stress is applied to the ligament. Over time, dogs with a steep slope, especially when combined with an upright stance, place enormous stress on the ligament, often resulting in tearing of the ligament. The ligament can also tear with twisting of the knee. When this ligament ruptures the whole joint becomes unstable, causing damage to the meniscus cartilages and eventually leading to osteo-arthritis.
Cruciate ligament rupture usually results in sudden lameness of one of the hind legs. The initial lameness will improve with time, especially if treated with anti-inflammatory medications.
However, due to progressive damage to the meniscus and the osteo-arthritis that will develop in the knee, the leg will get progressively lame again. The cruciate ligaments never heal, therefore, surgery is indicated for most patients.
The treatment of cruciate ruptures in dogs has developed over time with new techniques attempting to balance the forces in the stifle to reduce the abnormal movement in the joint.
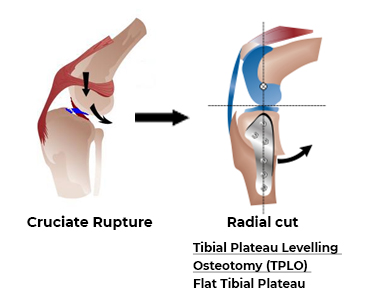
The most common procedures used at the moment are the Tibial Plateau Levelling Osteotomy (TPLO) and the Tibial Tuberosity Advancement (TTA).
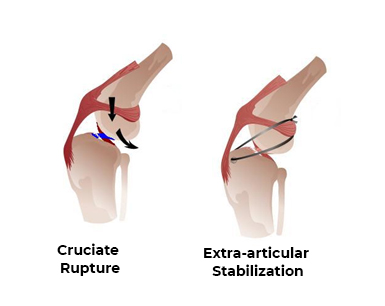
A fairly new development is the replacement of the ligament with a very strong synthetic ligament (Vetlig). Then there are still some techniques using some strong material on the outside of the stifle to limit the abnormal movement (Extra-capsular stabilization, AKA a Lateral Suture)
Before embarking on any surgical treatment, it has to be remembered that surgery is aimed at stabilizing the forces in the joint and slowing down the osteo-arthritis (OA) that develops in a joint if the joint has been injured. Most dogs will recover very well, but some degree of OA will always be present. Some dogs have advanced osteo-arthritis by the time that the diagnosis of cruciate disease is made and will have less dramatic improvement with surgery.
Tibial Plateau Levelling Osteotomy (TPLO) or Tibial Tuberosity Advancement (TTA
These techniques allow the dogs to regain good range of motion of the knee, keeping good muscular development as well as slowing the progression of osteoarthritis. Most importantly they allow the return to good function, depending on the pre-operative degree of degenerative joint disease.
At the moment we mostly do Tibial Plateau Leveling Osteotomy. Your dog’s surgeon will make a decision which procedure is the best option.
Before the actual surgery, we will give a sedation or a general anaesthetic to allow us to do a thorough examination of the knee and to take the necessary radiographs. The radiographs are assessed by the surgeon and the angles of the tibia are calculated to advise the most appropriate treatment.
Tibial Plateau Levelling Osteotomy
This technique involves cutting the top of the tibia, tilting it and fixing it in a new position with a plate and screws so that there is virtually no slope The biomechanical effect of the Tibial Plateau Leveling Osteotomy procedure (TPLO), is that the femur will no longer slide backwards on a steep slope, but will butt against a perpendicular surface, thereby taking away the need for the cranial cruciate ligament. There are different techniques to achieve a level tibial plateau. We use the radial cut technique.
Tibial Tuberosity Advancement
The TTA procedure involves making a straight cut in the front part of the tibia bone (tibial tuberosity) and advancing this portion of bone forward in order to realign the patellar ligament so that the abnormal sliding movement within the knee joint is eliminated. A specialized bone spacer, plate and screws are used to secure the bone in place. Bone graft is collected from the top of the tibia and placed in the gap in the bone to stimulate healing.
The surgery
Morphine, nonsteroidal painkillers and antibiotics are given at the time of surgery. The anaesthetic agents we use, namely propofol and isoflurane are among the safest drugs available.
The joint is opened and inspected for damage of the meniscus, which is treated by partial meniscectomy or meniscal release. The corrective surgical osteotomy is made in the bone, after which it is fixed in place at the correct angle with a surgical bone plate and screws. The operations take about one and a half to two hours.
The patient is closely monitored during surgery and as they recover. We like to keep most TTA and TPLO patients for one day post operatively to monitor progress.
Complications are possible following TTA or TPLO surgery, but are rare. Anesthetic reactions are extremely uncommon and rarely result in mortality under the care of trained personnel. Although infection may develop in the surgical site, this is uncommon, as strict sterile technique is used during the surgery.
If your dog is receiving medications such as chemotherapy or steroids the bone may not heal well, therefore it is imperative that you inform the surgeon prior to surgery that your dog is receiving these medications.Overexertion in the postoperative period may also result in poor bone healing, loosening of the screws or breakage of the implant.In addition, if your dog falls, the tibia may fracture. Arthritis (bone spurs) is usually present at the time of diagnosis of a cruciate ligament rupture and likely will progress regardless of surgical procedure performed.
If the arthritis symptoms progress, medications can be used to help relieve these signs. Reports indicate that there is about a 9 to 10% risk of developing a meniscal tear after surgery. Although some surgeons do a meniscal release to prevent this complication from happening, we prefer to keep the meniscus intact as it is an important structure in the knee function. Any dog that develops a sudden deterioration of symptoms, or has an audible click sound during movement of the knee, should be examined by the surgeon.
Post Operative Care and Rehabilitation at Forest Vets
After the surgery you can continue to give your pet prescribed pain relievers to minimize discomfort. Many dogs will soon use the leg, as the fixation is very stable. Although the fixation is stable, it is not strong enough to withstand use of the leg. Severe restrictions therefore have to be imposed during the bone healing process for six to eight weeks post operatively to avoid complications that could compromise the final results. Although some movement is good for maintaining joint mobility, the dog must be controlled at all times. No playing, jumping or running is allowed. When leaving the dog unsupervised they must be in a confined area, small room, cage or kennel. When outside, they must be on a lead.
Rehabilitation after TPLO or TTA
After the initial six-to-eight-week period, the dog’s exercise - rehabilitation can begin. During this time a gradual increase in duration of exercise will help build muscle. Be careful to observe the reaction to the exercise. While your dog remains comfortable you can gradually increase the duration of exercise but any signs of pain and discomfort you must allow rest and then return to last comfortable level of exercise.
VETLIG
A recent development is the placement of a very strong synthetic ligament as replacement of the cruciate ligament. The ligament is anchored in the joint with special bone screws which give immediate stability of the joint. Use of the leg is possible very soon after the surgery, when the pain of the surgery is controlled, so no stringent confinement is required for such a long period. Limitation of activity is required for about 10 days for the wound to heal, with lead walks for another 8 weeks.
This is the ideal method for older dogs, where bone healing may take quite long. It is also advisable when crate resting of a dog after the surgery will be difficult.
Although this is probably close to the ideal treatment of cruciate ruptures, there is a risk of infection in 5-10% of cases, despite taking extreme caution during and after the surgery. Although some infected cases can successfully be treated with antibiotics, as the material can protect bacteria, the ligament may have to be removed and another method used to stabilize the joint.
Extra-capsular stabilization using polypropylene or poly-amide
Although this method is probably not the ideal method of stabilization in heavier dogs, it has been successfully used in dogs as big as 25kg. It is the most effective in small dogs with an acute rupture of the cranial cruciate ligament, without a severe slope of the tibial plateau. It is not indicated in dogs with chronic arthritis or in very active dogs.
The advantages of this technique are the following:
- Cheaper
- Less risk of complications due to implant failures
- Less stringent post-operative restriction is required.
The disadvantage of this technique is that it does not address the forces acting on the joint, and may result in more osteo-arthritis developing in the joint. It can also fail, causing frustration and the need for further surgery.
The post-operative care of this procedure differs in that the dogs only have to be restricted for 2 weeks after surgery until the wound has healed. The polypropylene that stabilizes the knee is effective immediately and the dogs can use the leg quite soon. Some dogs take a couple of weeks to use the leg properly again due to wound healing and the osteo-arthritis.
References
- Hoffman DE, Miller JM, Ober CP, et al. Tibial tuberosity advancement in 65 canine stifles. Vet Comp Orthop Traumatol 19:219-227, 2006
- Lafaver S, Miller NA, Stubbs WP, et al. Tibial Tuberosity Advancement (TTA) for stabilization of the canine cranial cruciate ligament deficient stifle joint: Surgical technique, early results and complications in 101 dogs. Vet Surg 36:573-586, 2007
- Apelt D, Kowaleski MP, Boudrieau RJ. Effect of tibial tuberosity advancement on cranial tibial subluxation in canine cranial cruciate-deficient stifle joints: an in vitro experimental study. Vet Surg 36:170-177, 2007
- Miller J, Shires P, Lanz O, et al. Effect of 9 mm tibial tuberosity advancement on cranial tibial translation in the canine cranial cruciate ligament-deficient stifle. Vet Surg 36:335-340, 2007
- Boudrieau RJ. Tibial Tuberosity Advancement (TTA): Present Evidence. Proceedings of Annual Conference of the American Chapter of Veterinary Surgeons, October 17-21, 2007; p 312
- Maquet P. Advancement of the tibial tuberosity. Clin Orthop Relat Res. Mar-Apr:225-30, 1976
- Karlsson J, Lansinger O, Sward L. Anterior advancement of the tibial tuberosity in the treatment of the patellofemoral pain syndrome. Arch Orthop Trauma Surg. 103:392-395, 1985
- Karlsson J, Sward L, Lansinger O. Bad results after anterior advancement of the tibial tubercle for patello-femoral pain syndrome. Arch Orthop Trauma Surg. 111:195-197, 1992
- Cheng CK, Yao NK, Liu HC. Surgery simulation analysis of anterior advancement of the tibial tuberosity. Clin Biomech (Bristol, Avon). 10:115-121, 1995
- Montavon PM, Damur DM, Tepic S. Advancement of the tibial tuberosity for the treatment of cranial cruciate deficient canine stifle. 1st World Orth Vet Congress 2002; 152